As I write this I am sure there may be some other patients that will disagree with me. One of my challenges throughout this illness has been figuring out who I am now. I read a description of a person with a chronic illness as forever walking down a dividing line between the past and the future. Looking backward, he can see everything the illness has taken from him or has forced him to relinquish. Looking forward, he can’t see anything quite clearly. There’s no going back to the past, and the future is uncertain.
My story is my own and I accept that some of the things that define me now are not the same as others following their own path. For me, my life changed a lot during this illness. Being misdiagnosed for many years, as many others have been, we either dealt with the symptoms, or we sought out medical advice to find the answers. With a non functioning pituitary tumor that took years to grow, the changes in me happened so gradually that for most of my friends and family, they didn’t notice. It wasn’t until the last couple years that people could say they actually saw the changes in me. Changes that I didn’t notice myself.
Loss of aggression was one of the first major clues. Which sounds OK but in the construction business world you need aggression to deal with consultants and contractors on a daily basis. Loss of sex drive. This happened really over a couple years on a slow decline until i felt I was no longer functioning as a man or husband. It was the most difficult thing to admit and what finally got me to see my doctor. It was then that I was told at the age of 44 my testosterone was nil. The good thing was my doctor did not just prescribe me testosterone and leave it at that. He said to me, yes your testosterone is nil but we need to know why. Thankfully he sent me to an endocrinologist that completed the testing and found the golf ball tumor on my pituitary gland. Anyways you can read about all that in some of my previous stories.
For 12 years before being diagnosed I pushed my life to forward my career and provide for my family. I spent 70% of my working life traveling on the road for many years. In the last few years, I had worked my way to managing those people that would now spend their days travelling, and I had the chance to slow down and spend time at home. I had built an addition on the home for my wife to build her own business. Our future was planned and I had goals and dreams to pursue. We had been married for 22 years when the tumor diagnosis was found.
I wrote this to discuss the loss of identity. During the last, I would guess, two to three years before diagnosis, I made many mental mistakes with my life. I began to lose who I was. I can blame my hormone levels for being in the toilet if I choose. Really I don’t know. I gave up a career because I was struggling mentally but didn’t know why. I assumed I needed a change after so many years so I decided to start my own business. My marriage struggled. The mental challenges continued during this period until being diagnosed six months after giving up my career. They say everything happens for a reason…I am still trying to figure out the reasons.
Six weeks after surgery to remove the 4 cm tumor from my head, my wife tells me she wants a divorce. It destroyed me. I would love to tell everyone that I took it like a man and sucked it up and moved on. Truth is, being deficient on all hormones, adrenals, thyroid, growth hormone, sex hormones…I was a basket case. It was at this point that I lost who I was. Along with my identity, many other feelings came across. A loss of comfort, sexual function, career, income, self-efficacy, freedom, cognitive function, intimacy, pride, joy, self-esteem, self-control, independence, mental health, hope, dignity, and certainty. Over the last couple years I have felt these over and over again. Sorting though the grief alone is a tremendous challenge.
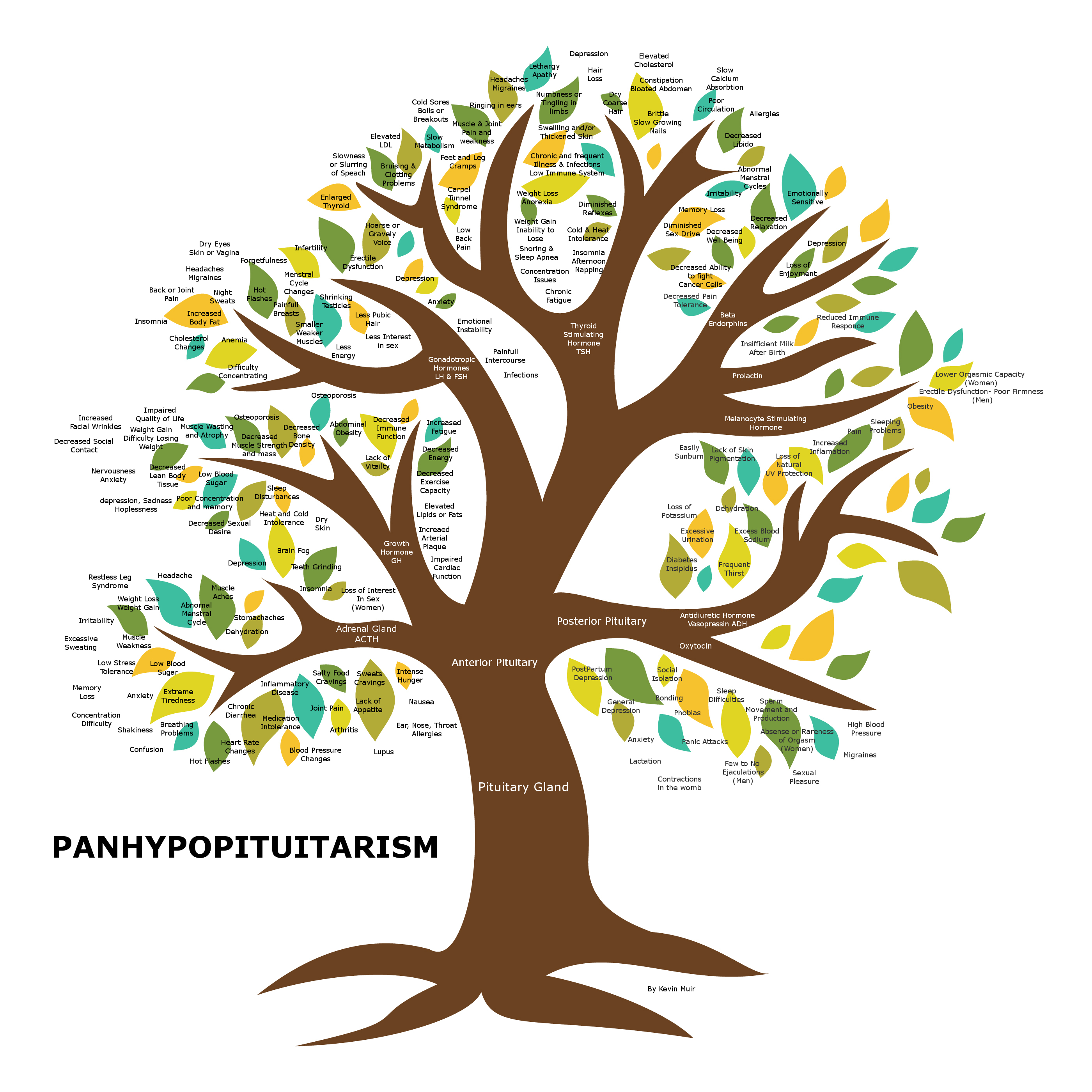
Until you yourself live through a complete hormone deficiency, you will never understand what those effects have on a person. My endo tried to describe it when replacing all these hormones synthetically that it was like going through a medically induced depression, puberty, menopause, and a mid life crisis all at the same time.
When you go through a tumor in your brain, many people you thought you were close to will step away. They don’t mean to be rude or not sympathetic but they don’t understand and it puts them face to face with their own mortality. They do’t know how to face you or what to say. Going through this tumor, plus a divorce, seemed to disconnect me even further. I went from the career guy with family and lots friends to the sick separated guy feeling alone and on my own to deal with this. I know people going through divorce normally go through some of these feelings. It was just magnified for me with the illness.
It was something that everyone I knew would never understand. You tell them it’s hypopituitarism and you get the blank stare. I was no longer the person that they used to know.
It has been almost three years now, since my original diagnosis. Tumor was removed in Oct of 2013. It has been two years of trying to synthetically replace all the hormones that others create on a regular basis but we have to balance and figure out correct dosages regularly. As much as I have tried to explain to family and friends, they will never truly understand what we work through daily. Yes…”I am fine”…I tell them. “All good!” What else can I say? I don’t want their pity and I don’t want them to watch me struggle. It’s written on the inside of my face. For people who are hypopituitary, our losses are multiple and permanent and therefore difficult to explain. They are infinite losses that will effect our quality of life forever.
Well-meaning individuals, whether friends and family or even doctors can make it more difficult. Some may try to add a helpful perspective by saying, “It could be worse” or “You look fine!” All these statements do are invalidate our physical and emotional challenges. It is very dismissive of the pain we are experiencing and the type of grief we are trying to manage. Everyone has a right to how they feel, and for us we just say, “It could be better.” There’s also a lot of pride in those of us with chronic illness and it makes us reluctant to ask for help from friends or loved ones. Sometimes we live in denial about our own limitations. We often retreat from our social networks, leading to poor social support. Our relationships will often suffer as we become more and more isolated. The depression can worsen to the point where some hypopituitary patients become actively suicidal or passively suicidal or just stop taking care of themselves in any meaningful way.
I gave up a while ago trying to explain the bad days because I really can’t explain them to myself. I am glad they have become fewer and further between than before. But how do you even try to explain when hormones are out of whack one day, but good the next? You can’t explain what its like to have your brain in a fog, pain in your body, emotional disconnect from others, a want to just be alone and a want to just be with someone that understands.
I have forgotten much of the year during diagnosis and have been trying to rebuild since then. I truly don’t believe all of the pieces are back in place yet. I am doing my best to move forward anyways but have yet to truly define or figure out who I am now. I know I am no longer the same person mentally that I was before this tumor. I seem to remind myself on a daily basis of this. It doesn’t make me less of a person. I probably help more people now that I ever did before because after going through this we find a connection with others that we never had before. My challenge is finding connection outside the illness itself.
In reviewing the psychology of this illness, I came across Maslow’s hierarchy of Human needs, he used the terms “physiological”, “safety”, “belongingness” and “love”, “esteem”, “self-actualization”, and “self-transcendence” to describe the pattern that human motivations generally move through.

What he says is there may not be any physical indications, but if a person is not meeting the most fundamental “physiological” needs as mentioned above, and “Safety” we can go through anxiety, tension and depression. The next most basic level of needs, Maslow called “deficiency needs” or “d-needs”: love, belonging, esteem, friendship, and physical needs and finally self actualization. Maslow’s theory suggests that the most basic level of needs must be met before the individual will strongly desire (or focus motivation upon) the secondary or higher level needs.
When you think about most of us that are diagnosed hypopituitary, we spend a countless amount of time searching and trying to understand our illness. Trying to find answers to why and what is causing all of our challenges. This is all part of the physiological state. Our next phase is security. Whether that be in finally finding a balance with hormones or finding a doctor/endocrinologist that understands or is willing to listen or help. Or having a partner or family member that is by your side for the duration and willing to love you no matter the challenges. Or just a feeling of finally understanding our own illness and how to read our own bodies needs.
Finding the next step for me has been difficult. A “love/belonging” or need. The belonging or need came through the support groups. I found peace and understanding with those going through the same as myself. Helping others going through this illness as I have, became what drove me day in and day out. But I am not fulfilled.
But I find myself still in this stage. Somewhere trying to sort out love and passions. What does it mean? What does it feel like? Why don’t I feel this? Why is there such a disconnect? Somewhere between here and the next stage, working towards my own self esteem, is where I seem to be stuck.
The human mind and brain are complex and have parallel processes running at the same time. Maslow said that the different levels of motivation could occur at any time in the human mind, but he focused on identifying the basic types of motivation and the order in which they should be met. Once we find that level of esteem again, we can move into the Self Actualization stage. Not everyone moves to this stage. Some choose to stay at the point that they have great self esteem and that is an amazing place to be.
“What a man can be, he must be. This need we may call self-actualization…It refers to the desire for self-fulfillment, namely, to the tendency for him to become actualized in what he is potentially. This tendency might be phrased as the desire to become more and more what one is, to become everything that one is capable of becoming.”
Self Actualization. To me this relates again back to finding my own identity. It’s no longer about comparing myself to who I used to be and trying to get back there again. I can only hope that one day I will be happy and find that new identity. I have to learn not to curse the storm but instead to learn to dance in the rain!